
Medical content has more of an impact when it is planned as part of a coordinated data dissemination strategy rather than treated as a series of isolated assets. For small and emerging pharma, that means connecting each deliverable to a shared scientific story, clear decision rights, responsible reuse, accessibility, and human-led scientific judgment so evidence can support the next decision, engagement, or data moment.
This article highlights several themes from the recently published MAPS white paper, Vision for Medical Communications 2035, and explores what those themes may mean for small and emerging pharma organizations that need practical structure without unnecessary complexity.
The “Asset-by-Asset Approach”: Death by a Thousand Cuts
Today’s medical affairs teams in small and emerging pharma are under pressure to do more with limited resources, evolving data, launch demands, and growing internal requests. In that environment, data dissemination strategy can take a back seat. Work quickly becomes asset–by-asset: a slide deck here, a congress summary there, a field resource, a digital update, a revised scientific narrative, or a version of a tactic for a new audience. Teams can lose sight of how each tactic fits into the broader scientific communication strategy.
To make HCP-facing content as effective as possible, each asset should support more than a single deliverable. Teams need to connect it to a shared scientific story, clear decision rights,1 and agreed rules for how evidence should be interpreted, adapted, reused, and measured.
The MAPS white paper identifies a shift that many lean teams are already experiencing: medical communications is increasingly expected to support ongoing scientific engagement rather than function solely as a process for developing individual deliverables. While the paper examines the future of medical communications broadly, many of the practical challenges look different in lean organizations with limited resources, fewer internal stakeholders, and less room for duplication or rework.
In small pharma companies, this shift is becoming visible in day-to-day work. Teams are now trying to connect emerging evidence, field needs, publication planning, digital behavior, and internal alignment goals to ensure that messages resonate meaningfully with the target audience. But what happens when data dissemination strategies have not been decided, agreed on, or communicated effectively?
The Signs Are Usually Easy to Recognize
When content development is underway, these problems occur:
- Scientific messaging differs in interpretation or is adapted differently across assets
- Publication plans, congress initiatives, field discussions, educational goals, and digital plans develop individually
- Review teams debate language late in tactic development because the narrative was not aligned early
- Teams duplicate efforts and rebuild content from scratch rather than leveraging existing, approved evidence
- Medical affairs stakeholders struggle to show how their communication efforts support the broader corporate strategy
In lean teams, these issues prove costly in various ways. They hinder decision-making, lead to rework, and make it more difficult to maintain a consistent narrative across publication planning, congress projects, field discussions, educational development strategies, and digital initiatives.
Building a coordinated data dissemination strategy starts with consistent, clear communication.
The MAPS paper describes an integrated medical communication strategy, or iMCS, as a more connected way to plan how evidence is communicated across audiences, channels, and time. For lean medical affairs teams, the practical value is straightforward: fewer disconnected decisions, clearer sequencing, and a stronger line of sight from evidence to action.
Right-sized Structure Matters
Small companies do not need or want big-pharma bureaucracy. But they do need structure to help teams move confidently.
A right-sized medical communications system makes content more impactful by giving medical affairs teams just enough structure to answer the questions that determine whether their strategy will be useful. These questions include:
- What are the core evidence points we need to anchor this year?
- Which data support each point?
- Which audiences need more context?
- Which assets should be connected, reused, or adapted?
- Who decides when the story changes?
- How will we know if our communication strategy made an impact?
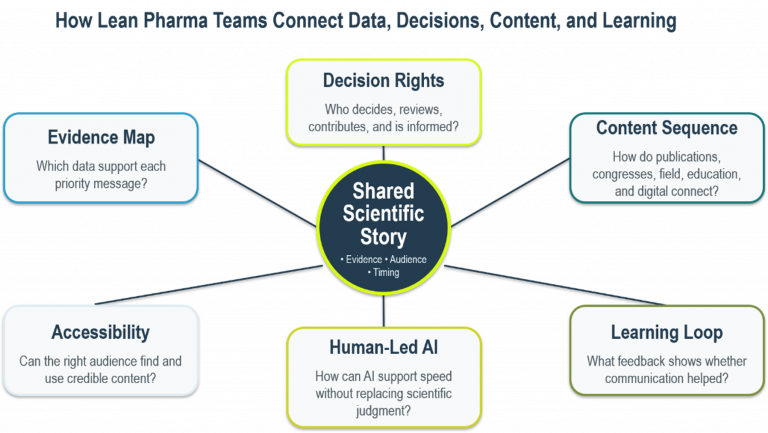
Figure 1. JB Ashtin’s right-sized system for connecting evidence, decisions, and communication.
Figure 1 presents JB Ashtin’s interpretation of several themes discussed in the MAPS white paper and how those concepts can be operationalized within lean medical affairs organizations. The framework shows how teams can connect evidence, decisions, content planning, accessibility, human-led AI, and learning around 1 shared scientific story.
Publications Should be Part of a Sequence, Not The Finish Line
Publications remain essential as peer-reviewed evidence still carries weight.
But publication planning should not sit off to the side as a separate activity. The MAPS paper points out that traditional publication timelines can be too slow for the current pace of science and that publication strategy is increasingly becoming one component of a larger evidence communication ecosystem.
A manuscript, congress presentation, plain-language summary, medical education activity, field resource, and digital asset should not feel like unrelated pieces of work. They should be connected by the same data interpretation and message strategy.
For small pharma, this is especially important because there may be only a few major moments (or pieces of data) to work with. If those moments or data are not planned as a sequence, momentum can be lost.
A stronger approach makes each content decision serve the larger sequence. The questions that need to be addressed include:
- What requires peer-reviewed publication?
- What should be prepared for congress discussion?
- What context will field teams need?
- What can be reused credibly and compliantly?
This is how publication planning becomes more than a timeline. It becomes part of a larger plan for helping evidence reach the right audiences with the right context, at the right time, in formats that can be extended responsibly.
Credible Scientific Information Needs to be Easily Accessible
HCPs get their information from more than just journals, congresses, or direct interactions. They search and evaluate information via many sources to stay informed and effective.
The MAPS paper highlights the growing role of digital formats in conveying medical information. It provides valuable insights into how HCPs discover content online, what channels they use, how content performs across platforms, and how search terms and digital formats influence access to information.
That does not mean medical communications should blur the line between credible scientific exchange and promotion. Instead, teams need to think carefully about whether credible scientific content is easy to access, easy to understand, and easy to use responsibly.
A team may have strong data, a thoughtful publication plan, and well-reviewed materials. But if the right audience cannot access the information, or if the content is not shaped for how HCPs seek answers, the scientific story may not reach its full value.
The goal is to make important scientific information clear, responsible, accessible, and available in the places and formats where the intended audience is likely to look, so strong content can keep working after the first use.
AI Can Help, But It Should Not Lead
AI is becoming part of pharma workflows, but it does not change who is accountable for scientific accuracy, balance, and judgment.
Used well, AI can help with literature summaries, content organization, draft development, workflow support, and quality checks. The MAPS paper appropriately positions AI as a support tool, not a substitute for scientific accountability. For small pharma, the practical takeaway is simple: AI may accelerate work, but people still own data interpretation, engage in critical thinking and analysis, and identify any potential risks. See our previous blog on adopting AI with human accountability for more on this topic.
For small pharma, this accountability means setting clear expectations:
- Source material must be verified
- Scientific review must remain human-led
- Claims must be checked against approved evidence
- Drafts need context, not just polish
- AI use should be documented where appropriate
- Speed should not come at the expense of trust
The future is experienced teams using AI carefully so they can spend more time on the decisions that matter.
Transforming Evidence Into Action: The Power of Medical Communications
One of the strongest points in the MAPS paper is that medical communications should have a clearer strategic role within medical affairs. For small and emerging pharma, that strategic role is practical: helping the organization translate data thoughtfully; align teams before external engagement begins; create consistency across congresses, publications, education, field needs, and digital content; and build materials that can be reused and adapted without letting the scientific story drift.
A strong data dissemination strategy does not have to be complicated. It should make clear what evidence matters, how it should be sequenced, which assets should connect, where reuse is appropriate, who has decision rights, and how the communication’s impact will be assessed.
An experienced partner can help teams organize the evidence, pressure-test the narrative, identify where messages may drift, and build materials that work across publications, congresses, education, field needs, and digital platforms without adding unnecessary complexity.
Strong medical communications can help lean teams turn evidence into coordinated action across channels by keeping scientific judgment in charge, using AI carefully, making evidence easier to understand and apply, and designing each HCP-facing asset to support the next decision or engagement.
¹ Clear decision rights help teams avoid late-stage debate by defining who decides how data should be interpreted, which messages are approved, how content can be adapted, when the scientific story changes, and which assets need to be updated.
Let's Build What's Next, Together
We know how crucial it is to get it right in medical communications. If you’re looking for a partner who can balance creativity with compliance and deliver impactful results –